











































Lessons Learnt in Scaling up Evidence-based Comprehensive Health Sector Responses Addressing Female Genital Mutilation in Highly Prevalent Settings
Affiliation
World Health Organization (WHO)
Date
Summary
"The multicountry engagement enriched knowledge sharing across countries and may have potentially saved resources and time..."
Affecting over 200 million girls and women, female genital mutilation (FGM) is a harmful practice that violates children's rights and the rights to health and bodily integrity. The aim of this practice paper is to describe a multicountry participatory approach that was initiated by the World Health Organization WHO in 2018 to facilitate the uptake and scale up of comprehensive health sector programmes in countries with high FGM prevalence. The paper describes the scale-up approach used, its key achievements from programmatic reports from 2018 to 2022, its strengths and weaknesses, and proposed areas to be strengthened in future scale-up efforts.
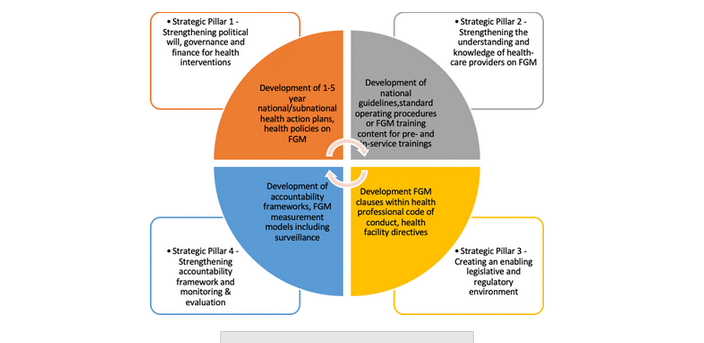
Pillars of action that guided the multicountry participatory process included: (i) strengthening the political will, governance, and funding for FGM-related health sector interventions; (ii) increasing the understanding and knowledge of health workers on FGM; (iii) creating an enabling legislative and regulatory environment; and (iv) strengthening monitoring, evaluation, and accountability. The 3-step process was composed of annual cycles where ministries of health and health stakeholders from priority countries developed comprehensive national action plans, implemented prioritised foundational activities using 8 WHO resources, and shared learning with other countries.
In 2018, 10 countries participated in a 3-day in-person meeting with 56 participants; in 2021, 13 countries participated virtually, with 70 participants; and in in 2022, 7 countries participated virtually, with 25 participants. Ten preliminary health plans were developed, out of which 7 were finalised. (Table 1 in the paper details the progress of countries that developed national action plans during 2018-2022.) During implementation, new knowledge was generated or gaps identified in guidance or evidence-based technical resources. The documentation of this learning generated a need to develop additional WHO guidance, such as a facilitator guide for person-centred communication for FGM prevention (see Related Summaries, below).
Other reflections on the scale-up approach include, for example:
In conclusion: "This scale up approach could be of use for other health topics that are relatively 'new' to the health systems as it creates motivation and comradery in tackling challenges and celebrating successes."
Affecting over 200 million girls and women, female genital mutilation (FGM) is a harmful practice that violates children's rights and the rights to health and bodily integrity. The aim of this practice paper is to describe a multicountry participatory approach that was initiated by the World Health Organization WHO in 2018 to facilitate the uptake and scale up of comprehensive health sector programmes in countries with high FGM prevalence. The paper describes the scale-up approach used, its key achievements from programmatic reports from 2018 to 2022, its strengths and weaknesses, and proposed areas to be strengthened in future scale-up efforts.
Pillars of action that guided the multicountry participatory process included: (i) strengthening the political will, governance, and funding for FGM-related health sector interventions; (ii) increasing the understanding and knowledge of health workers on FGM; (iii) creating an enabling legislative and regulatory environment; and (iv) strengthening monitoring, evaluation, and accountability. The 3-step process was composed of annual cycles where ministries of health and health stakeholders from priority countries developed comprehensive national action plans, implemented prioritised foundational activities using 8 WHO resources, and shared learning with other countries.
In 2018, 10 countries participated in a 3-day in-person meeting with 56 participants; in 2021, 13 countries participated virtually, with 70 participants; and in in 2022, 7 countries participated virtually, with 25 participants. Ten preliminary health plans were developed, out of which 7 were finalised. (Table 1 in the paper details the progress of countries that developed national action plans during 2018-2022.) During implementation, new knowledge was generated or gaps identified in guidance or evidence-based technical resources. The documentation of this learning generated a need to develop additional WHO guidance, such as a facilitator guide for person-centred communication for FGM prevention (see Related Summaries, below).
Other reflections on the scale-up approach include, for example:
- The adaptation of WHO resources to the country context in consultation with relevant stakeholders improved their relevance and acceptability.
- The multicountry experience-sharing created a community of practice to support implementation of FGM-related health interventions. The follow-up, mentorship, and bidirectional cross-learning and monitoring and evaluation improved the uptake processes too. However, WHO found very limited programme data to examine the impact of the comprehensive health sector approach on health workers and FGM prevention and care services for the countries that implemented foundational activities.
- The experience-sharing enabled bidirectional learning between countries and WHO. The involvement of three levels of WHO ensured global, regional, and in-country technical support, learning, and coordination. The close partnership in planning and implementation identified implementation areas that needed evidence-informed guidance.
- The COVID-19 pandemic affected the scale-up approach process. For instance, travel restrictions limited the in-person participation of WHO regional and headquarter staff to support in-country national planning exercises and implementation of activities. WHO found that the in-person multicountry and in-country meetings were more successful compared with virtual meetings in engaging participants.
- Identifying in-country leadership and champions or advocates to recognise and invest into FGM as a public health issue and increasing the numbers of in-country experts/mentors to disseminate and facilitate the adaptation of evidence-based resources during implementation;
- Monitoring implementation and impact of the FGM interventions to generate programmatic data systematically;
- Including wider stakeholders from other sectors involved in FGM abandonment efforts, as well as the private health sector, during multicountry and in-country health action plans development and evaluation meetings; and
- Increasing the frequency of multicountry experience-sharing meetings and documenting each country's experience as case studies to expand the learning and quality of the health interventions addressing FGM.
In conclusion: "This scale up approach could be of use for other health topics that are relatively 'new' to the health systems as it creates motivation and comradery in tackling challenges and celebrating successes."
Source
BMJ Global Health 2023;8:e012270. doi:10.1136/bmjgh-2023-012270.
- Log in to post comments