











































Strategies to Reach Nomadic Children During Polio SIAs: Experience in Dadaab and Fafi Sub-Counties of Kenya after the 2013-2014 Polio Outbreak
World Health Organization (WHO), Nairobi (Ahmed, Mohamed, Onuekwusi); WHO Regional Office for Africa, or WHO AFRO (Okeibunor, Mkanda); WHO Horn of Africa Coordination Office, or HOA (Okiror)
"...to achieve any meaningful success in a community level programme, identifying and engaging its key decision makers throughout is vital."
A nomad is a member of a people or tribe who according to the changing seasons moves from one place to another to meet the needs of their livestock. In most of sub-Saharan Africa, access to healthcare services by nomads is poor compared to settled populations. During the 2013 polio outbreak in Garissa County in Kenya, 50% of the confirmed cases were among nomads, even though they comprise less than 20% of the total population in the county. Following concerns from the Horn of Africa Polio Technical Advisory Group (HOA-TAG) regarding inadequate vaccine coverage of the nomadic population, several strategies were put in place to improve supplementary immunisation activity (SIA) participation and acute flaccid paralysis (AFP) case reporting among nomads for the rest of the planned 2014 polio vaccination campaigns. This article describes strategies initiated from April 2014 by the Ministry of Health (MoH) and partners to reach children in nomadic settlements in two sub-counties of Dadaab and Fafi of Garissa County. These two sub-counties were selected because six out of the seven cases reported from the nomadic population were located here.
Responding to the recommendations of the HOA-TAG and as part of the outbreak vaccination response, new initiatives were implemented, as follows:
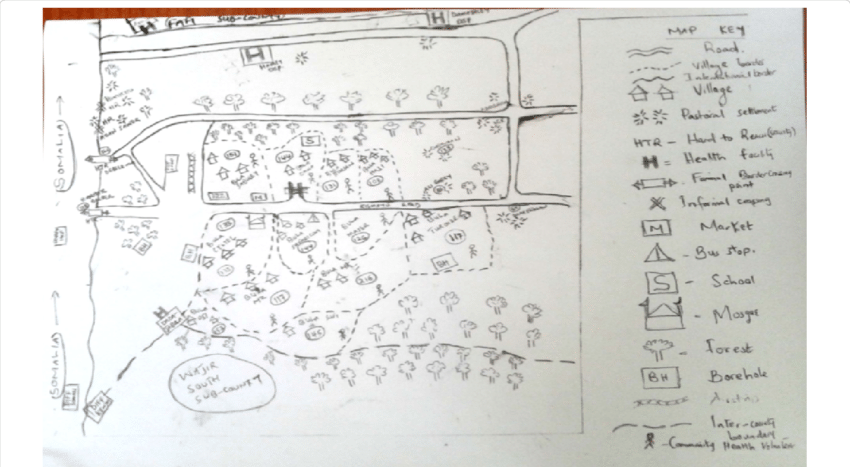
- The initial step was to create a list of nomadic settlements in both sub-counties based on information obtained from local clan elders and government administrators, which detailed under-5-year-old populations, available channels for social mobilisation, and focal persons. Specifically, from each settlement, a contact person was identified and then linked to the MoH polio campaign planning team. These contact persons, who were invariably male, were either living in the settlements or were family members living in trading or market centres within the area. They were engaged to mobilise residents in their respective settlements to support vaccine uptake and to guide vaccination teams during SIAs.
- During campaigns, the MoH planning team would select specific teams to reach these settlements. To reach children in settlements located far from main centres or where access was limited to motorised transport or by insecurity, community health volunteers (CHVs) drawn from the relevant clans and trained to give OPV were sent. Besides OPV, the teams carried with them basic drugs to treat common childhood illnesses they may find in the field. A tracking tool to monitor nomadic population movement and special tally sheets to capture data were created.
- From the start of the outbreak, attempts were made to reach out to the nomadic community to involve them in reporting suspected AFP cases. These initiatives started 8 months after the last confirmed case (July 2013) and were intended to ensure the continued participation of the nomadic population in AFP surveillance. Experienced CHVs were assigned to each listed nomadic settlement in the two sub-counties to sensitise the identified leaders and contact persons on the lay case definition and how to report a suspected AFP cases. Any suspected AFP case was to be reported to the nearest health facility.
About 2,000 additional children from both nomadic and non-nomadic areas were reached when the new initiatives were started. According to organisers, for the first time, an actual number of nomadic children accessed was documented. Suspected AFP cases continued to be reported from nomadic settlements, and - probably as an indication that more nomadic children were reached in the campaigns using the new strategies - 100% of the AFP cases reported from nomadic settlements in 2014 and 2015 had received at least one dose of OPV.
Per the paper's authors: "The takeaway lesson from this experience is that to maintain momentum in the implementation of such interventions, teams assigned for nomadic settlements need to be retained and retrained before each round and supervision strengthened to ensure proper data entry....[In addition, h]ealth management teams need to work closely with other sectors in order to leverage on their success in reaching all children in the area with vaccines."
In conclusion: "With modification and improvement, these strategies may be used to take health services such as routine immunisation to nomadic communities and reduce their vulnerability to vaccine preventable disease outbreaks."
Journal of Immunological Sciences (2021); S (002): 31-38.
- Log in to post comments